
 Today is the APA’s Annual Mental Health Blog Day. I’m diving into an aspect of Postpartum Mood & Anxiety Disorders which is often swept under the rug yet brings with it a very divisive and stigmatizing aspect to the birthing world. I dove into this topic somewhat with a blog post just a week ago, but today I’m diving in even further because beneath the exposure of THAT post, there is even more stigma and non-discussion going on among some of the largest birth support organizations (Lamaze, DONA, and CAPPA) in regard to Postpartum Mood & Anxiety Disorders.
Today is the APA’s Annual Mental Health Blog Day. I’m diving into an aspect of Postpartum Mood & Anxiety Disorders which is often swept under the rug yet brings with it a very divisive and stigmatizing aspect to the birthing world. I dove into this topic somewhat with a blog post just a week ago, but today I’m diving in even further because beneath the exposure of THAT post, there is even more stigma and non-discussion going on among some of the largest birth support organizations (Lamaze, DONA, and CAPPA) in regard to Postpartum Mood & Anxiety Disorders.
If you read the post linked in the above intro paragraph, you’ll read that Henci Goer’s view of Postpartum Mood and Anxiety Disorders places the blame for experiencing them on the breakdown of the system of medical intrusions into the birthing experience. If we could just fix the system, she believes, Postpartum Mood & Anxiety Disorders (which are all PTSD related to intrusive medical occurrences during birth, by the way), would disappear and every single mother would be just fine.
Only it doesn’t work that way. We could have the most perfect birth in the world and still end up with some form of a Postpartum Mood & Anxiety Disorder. I’ve talked to mothers who have had this happen to them. Do the intrusions add to the potential? Sure. It’s a risk. Know what else is a risk? Being female and being pregnant. Researcher after researcher has proven that while yes, there are actions we can take to alleviate our risks or shorten our experiences, we are ALL at risk regardless of our stature in life or the manner in which we give birth. From those at the highest of society (Kim Kardashian, anyone?) to a woman in a third world country with the most meager access to care, we are ALL at risk. Different language may be used to express those experiences, but going “mad” after childbirth is something which has occurred since the time of Hippocrates and doesn’t show any signs of slowing down.
I’m not saying that we are all DOOMED to experience Postpartum Mood & Anxiety Disorders, absolutely not. I’m saying that our risk factors are similar. Additional stress adds to our risk weight but beyond that, pregnancy itself is a risk factor as it does things to our bodies, to our hormones, to ourselves, that we will never fully understand regardless of how much research we do. The best way, I think, to approach pregnancy, is to advocate for the best care for yourself, whatever that may be. If you need an epidural to give birth, then go for it. If you want to give birth naturally, go for it. But be aware that birth is a fluid and organic process over which we truly have no control. Things may happen for which we are either not prepared or not willing to have happen. However, if you’re open to the possibility that they *may* happen, the result may be less traumatic and therefore leave a shorter impression upon your psyche.
In reading through Lamaze’s Listening to Mothers III report, I’m hit with some thoughts about how well the birth community IS listening to mothers. So I decided to go hit some of the other websites to see where they stand on Postpartum Depression Mood & Anxiety Disorders. How well do they prepare Mothers for the possibility of these issues and/or how well do they welcome mothers who have birthed before and experienced these things and are now searching for a “better” way to birth in order to avoid similar issues?
The answers were not good.
ACOG, the American College of Obstetricians and Gynecologists, has a published Opinion Paper on Screening for Depression During and After Pregnancy. It was issued in 2010 and reaffirmed in 2012. This opinion includes a chart mentioning several different methods of screening, notes the amount of time it takes to go through each one, the sensitivity of the screening method, and if it’s available in Spanish. ACOG then concludes by saying the following:
“Depression is very common during pregnancy and the postpartum period. At this time there is insufficient evidence to support a firm recommendation for universal antepartum or postpartum screening. There are also insufficient data to recommend how often screening should be done. However, screening for depression has the potential to benefit a woman and her family and should be strongly considered. Women with a positive assessment require follow-up evaluation and treatment if indicated. Medical practices should have a referral process for identified cases. Women with current depression or a history of major depression warrant particularly close monitoring and evaluation.”
Not only do they recommend screening, they recommend development of a referral process AND note that women with current depression or a history thereof should be monitored. Kudos, ACOG.
DONA has several position papers available at their website. The one for the Postpartum Doula does not mention Postpartum Depression aside from the following sentence:
DONA also offers up a Postpartum Plan worksheet for new mothers. Nowhere on this sheet does it at all mention what to do if a Postpartum Mood & Anxiety Disorder appears. To DONA’s credit, however, there are books included on their required reading list for their Postpartum Doula Certification by known Postpartum Mood & Anxiety Disorder experts. The books, however, are older, and the PDF for Postpartum Doulas has not been updated since 2009 while the list for the Birth Doulas was last updated in 2013.
CAPPA’s position paper for Postpartum Doulas makes mention of Postpartum Depression and focuses on the “fourth trimester” as one which must be traversed as carefully as the three trimesters of pregnancy. The Postpartum Doula, according to CAPPA, is not to provide medical care, but to have a network of caregivers (none of which are therapists, psychologists, or psychiatrists) which they can refer the family to if so needed.
According to CAPPA, the Postpartum Doula does the following:
“Postpartum doulas are knowledgeable professionals who assist families during the critical period immediately after the birth of their baby. They “mother the mother” and offer physical, emotional and informational support to the family as well as practical help.”
Makes sense, yes? After all, we do need to be mothered after giving birth. We know how difficult it is to make that adjustment to having the baby on the outside instead of on the inside.
The reading list for the Postpartum Doula at CAPPA has only three Postpartum Mood & Anxiety Disorders books listed, two less than DONA. The Childbirth Educator certification list has NO books regarding Postpartum Mood & Anxiety Disorders.
In discussion with various OB’s, I’m told they spend less than 2 weeks on Postpartum Mood & Anxiety Disorders as they train for their specialty. Two weeks to understand the complexities of Psychiatric issues post-birth.
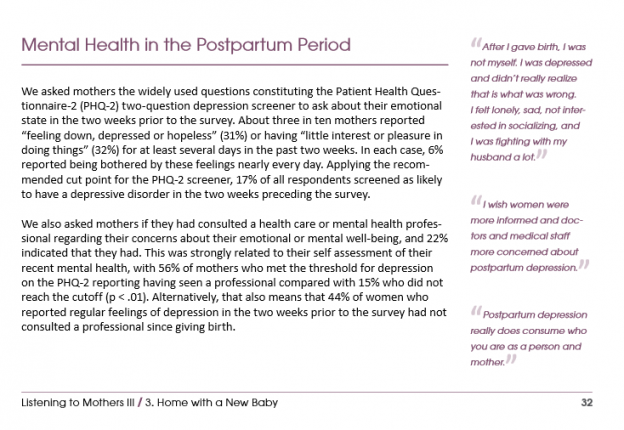
Bringing things full circle, the Lamaze Listening to Mother’s III report has this to offer about Postpartum Mood & Anxiety Disorders:
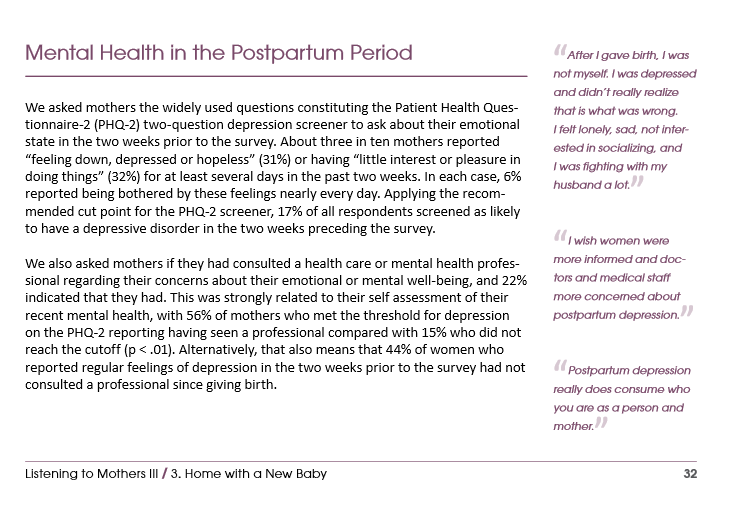
I don’t know what’s more disturbing here – that 31% of the mothers were self-reporting as feeling down or depressed or that 44% of these women with regular feelings of depression in the two weeks prior to the survey HAD NOT CONSULTED A PROFESSIONAL SINCE GIVING BIRTH.
Going back to my article about Henci’s comment at a previous post over at Science & Sensibility, you’ll note that she mentions “Furthermore, on-site mental health services would be of little use to women suffering from childbirth-related emotional trauma because one of the prime protective responses is avoidance of environments and personnel that re-trigger traumatic memories.”
I cannot help but wonder if the training, the discussions, the passing down of the believe that if only your birth is perfect and free of all possible interventions (as is impressed upon by the Lamaze Healthy Birth Practices found here), you’ll be just fine attitude held by so many within the birthing community is……
HINDERING MOTHERS FROM SEEKING HELP?!?!?
There are the standard reasons, of course, lack of insurance (due to Medicaid), cost, transportation, childcare, stigma/denial from family members, etc.
But what if… what if this stigma and denial is also coming at women from their caregivers? I know I had it from my OB. I know women who have been told horrific things when they’ve managed to call for help – things from “Well, are you suicidal yet?” to “Oh, just go shopping or take a walk and you’ll be fine…” or what I heard which was “Your hormones slid back into place at 4wks postpartum so this can’t be Postpartum Depression.”
I’m pleading with the caregiving community as a whole – with Obstetricians, with midwives, with pediatricians, with doulas, with anyone and everyone who may come in contact within a medical capacity with a pregnant or new mom to accept what she has to say as truth. To not try to reframe it for her, to not brush it off, to not dismiss her very valid fears and concerns. Listen. Truly listen. Don’t run through all your evidence based research in your head as she’s pouring out her heart to you – because if she’s doing that, it took her a very long hard look inside to be able to do that and if you say the wrong thing, you’re going to shut her down very quickly and do harm to her recovery process.
For those who DO listen, who do educate themselves and go beyond the certification recommendations, thank you. Thank you for bringing awareness to this struggle that so many of us fight.
With every birth, a new mother is born. It does not matter if she’s been born into the role before, she is reborn with each child. For each child and each aftermath presents a different set of challenges with which she must learn to live. Be gentle. Be kind. Be supportive. Listen. Don’t shame. Don’t stigmatize. The trust of a new mother is an amazing thing.
Stop abusing it, stop re-framing it, and above all else, wrap it in love and return it with your own level of compassionate honesty.
We, the women of the world, the mothers of all of you, deserve at least that much.
 Tell us a little bit about yourself. Who is Mary Jo Codey when she’s not passionately speaking out about Postpartum Mood Disorders?
Tell us a little bit about yourself. Who is Mary Jo Codey when she’s not passionately speaking out about Postpartum Mood Disorders?  Are you excited?
Are you excited?